Cortisone shots are a common therapy that doctors frequently rely on when facing conditions like tendonitis and plantar fasciitis. But does cortisone really work?
I’ll try to answer that question in some depth in just a minute. But let’s start with what cortisone actually is.
First and foremost, cortisone is a hormone that’s produced by the adrenal glands. To be specific, it’s a cortico-steroid (not to be confused with anabolic steroids, which are what professional – and a lot of recreational – bodybuilders use to increase their muscle mass), and the cortisone produced by your body is absolutely essential if you want to maintain proper function and health. There are a few unfortunate folks who have a condition called Addison’s Disease, but aside from them cortisone is naturally produced by every human being. This means that no one has any allergy issues with the substance.
If you decide to get a cortisone shot, your physician usually won’t load it up with the pure stuff, which has a short period of effectiveness (and isn’t especially potent). Instead, more generally prescribed alternatives are derivative compounds made from actual cortisone. These compounds are longer-lasting and burden the patient with fewer side effects. In most cases, there is some sort of pain-relieving substance in the shot, too.
Cortisone generally works well to alleviate inflammation, at least for short periods. This naturally provides a certain amount of relief, but at the same time doesn’t really help to cure the root cause of the problem. In the end, your pain will come back once the effects of the shot wear off. There is also a limit (and a pretty low limit, at that) to the number of shots you can get inside a given time period. Animal research has shown that cortisone can actually weaken whatever tendon or fascia it’s applied to, especially if it’s injected too often into a local site.
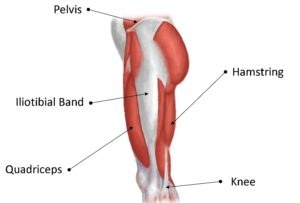
This possible, but very frequent, antagonistic effect is a problem more in younger people than older ones, because younger tendons and fascia are still relatively healthy. Patients up to the age of around twenty-five or thirty should attempt other types of treatment before choosing a cortisone shot. Older patients, on the other hand, who have joints that are almost always already somewhat damaged, don’t need to be as concerned. There are also particular tendons and fascia that have a high frequency of tearing even when the cortisone shots are given as carefully as possible. The Achilles tendon in the back of your heel is a prime example. Cortisone shots given there will make the tendon more likely to tear rather than less, because of the extreme stress placed on the foot and ankle during walking, running and jumping. Not only do you have your entire bodyweight come down on the tendon, if you’re moving fast the force can be multiplied many times over.
Physiologically speaking, inflammation is a useful reaction in most cases. But it can also turn into something counterproductive, actually hindering the healing process when you get too much of it. A cortisone shot is supposed to suppress unnecessary inflammation, which in turn helps the body heal itself. But increasingly, modern research is tending to show that chronic, long-term conditions like plantar fasciitis and tendonitis are not actually the result of inflammation but some other mechanism. (The most likely suspect is thought to be direct damage to the primary tissues, which would technically make it plantar fasciosis or tendonosis. You can check out this article for the difference between an ~itis and an ~osis.) Of course, this means that the reason for administering a cortisone injection is a little sketchy in the first place.
So why do patients frequently report a lessening of pain when they get a cortisone shot? Well, first of all not everyone does; statistics show that the injections only prove effective about half the time. But a fair percentage of patients do experience a significant degree of relief, the most likely reason being that the analgesic in the shot is temporarily masking their pain. And, of course, there’s always the possibility of a placebo effect.
I don’t want to come off as being totally anti-cortisone here. Cortisone can be an absolutely great option in certain cases. In fact, if you’re an older patient suffering from arthritis it might even be your best choice. But when it comes to conditions like fasciitis/fasciosis, there are some real doubts concerning its efficacy. Particularly with younger patients, but also with older ones as well, it appears that there really are less invasive and more effective treatments… ones that have both a higher cost-benefit ratio and a significantly higher percentage of success.
So to return to the original question, does cortisone really work? Here are the major advantages to getting a cortisone shot:
First, the injections are relatively inexpensive. Second, most insurance plans will cover them. Third, they’re quick and easy to get. And fourth, doctors can keep a close eye on their effects.
Now for the disadvantages:
One, having a needle stuck directly into damaged tissue (I’ve had this done, and believe me, it hurts). Two, possible side-effects that may end up requiring surgery. Three, the questionable way that cortisone is supposed to work, and four, the coin-toss number of people who experience even short-term relief.

Looking at the above, you might get the idea that there are mostly economic and convenience advantages, while the disadvantages are mostly physical. (And you would be correct.) It’s a case-by-case decision, of course; some people have no choice but to place more priority on their wallets than a possible hit to their health. But if you’re in a position to put more emphasis on your health, I think it’s just common sense to want to give other treatment options a chance first.
Fortunately, there is at least one alternative treatment that will run you less money than a regular visit to your doctor. If you have long-term plantar fascia or tendon pain and haven’t been able to get rid of it, the first thing to do is take my free, one-minute test to see what your real problem is (an ~itis or an ~osis). Assuming you have fasciosis/tendonosis, my program will pinpoint the root cause of your condition, doesn’t require a doctor’s supervision, is completely safe and can be performed more or less anywhere at any time. Not only that, 100% guaranteed for 60 days. If this interests you, take a moment and click on the link above.